202530 Three enclosed space fatalities
Providing learning through confidential reports – an international co-operative scheme for improving safety
An anchored bulk carrier was preparing to load coal. The chief officer and a surveyor completed the ship-shore safety checklist and a floating crane was secured on the bulk carrier’s starboard side to load coal from open barges towed from shore.
Loading was planned to take place into nine cargo holds over eight days or more. There were frequent stops due to barge logistics and heavy rain showers that required the hatch covers to be closed to prevent the cargo becoming saturated.
On day 8, the twentieth barge came alongside at 0320. Loading into cargo hold No.7 resumed at 0325 and continued until 0630, when a bulldozer was lifted into the hold to trim off the cargo. At 0830, the daily testing of hold atmospheres was completed through the testing point on the hold hatches using a portable gas detector. Cargo hold No.8 was noted to have 8% lower explosive limit (LEL) methane, 225 parts per million (ppm) carbon monoxide, and 5.8% oxygen.
At 0840, heavy rain caused cargo work to be stopped, and about 20 minutes later all cargo hatches were closed. Bulldozer operator 1 left the bulldozer in cargo hold No.7 and exited the hold. At about 1236, bulldozer operator 2 arrived on the bulk carrier’s main deck. As the rain had stopped, he asked the foreman to have the hatch cover to cargo hold No.7 opened to complete the trimming operation in the hold. The foreman relayed the request to the vessel’s duty officer by VHF radio.
Soon after the call, crew opened the hatch of cargo hold No.7. CCTV cameras on the vessel’s main deck recorded bulldozer operator 2 making several solo entries into the cargo holds. At about 1305, the assistant foreman went to check on the progress in cargo hold No.7 but could not hear the bulldozer working. He checked the main deck surrounding cargo hold No.7 before returning aft. Further checks failed to find the missing bulldozer operator.
Some minutes later, the assistant foreman entered hold no 7 via the forward booby hatch to continue looking for bulldozer operator 2. Still unsuccessful, he climbed onto the port side hatch coaming of hold No.7 and walked aft, pausing to check the hold as he went. Seeing that hold No.8 forward booby hatch was open he went over to look inside. He saw bulldozer operator 2 lying apparently unconscious in the access space on the deck below.
The assistant foreman immediately raised the alarm. Crew gathered, and the 2/O told the assistant foreman that no one should enter the space. The 2/O and two crew then ran to retrieve the ship’s rescue equipment, which included breathing apparatus (BA) sets.
By this time, about six stevedores had assembled by the booby hatch. At 1329, a stevedore and the foreman descended the ladder into cargo hold No.8 forward cargo access space to try to rescue their colleague. Within seconds they collapsed unconscious. Three minutes later, the bulk carrier’s rescue team arrived on scene and saw that there were now three casualties in the space. After testing the atmosphere, the rescue team entered the access space with BA gear. Within nine minutes all three victims had been brought to the main deck. Cardiopulmonary resuscitation and oxygen were administered but none of the victims regained consciousness. The victims were transferred ashore where they were later declared deceased.
The investigation found, among other things, that none of the victims had completed enclosed space awareness training. Post mortem examinations were not conducted, and the cause of death was not confirmed. However, atmospheric readings taken at the forward access space to cargo hold No.8 after the accident show a deficiency of oxygen and a high level of H2S. It is highly likely that the noxious air caused the victims to become incapacitated upon entry into the cargo access space, and the resulting accelerated shutdown of their brain and/or lungs led to their death.
Lessons learned
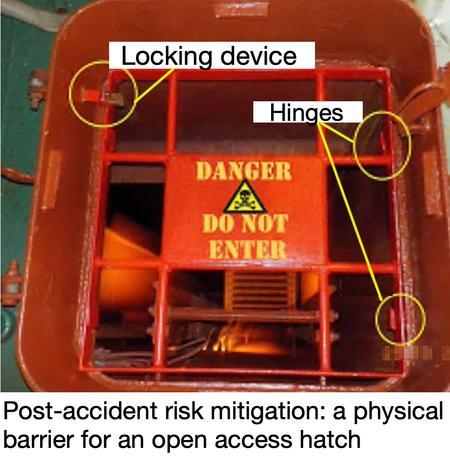
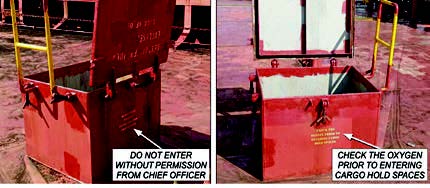
- Effective access control, either by a physical barrier or robust entry procedures that prevent easy access to hold spaces, will reduce enclosed space casualties.
- Enclosed space awareness training for stevedores will enhance safety on vessels.
- A false sense of security is easily set in place. In this instance, there had been many days of loading with less than adequate control over hold access with no apparent consequences. Then disaster struck – a stevedore entered hold 8 which had noxious gases. As rescue operations were mustered, less than adequate ‘accident scene control’ allowed two more fatalities to occur.