
202122 Crane crush fatality
As edited from MAIB (UK) report 18/2020
A general cargo vessel finished loading a cargo of cement in the early morning hours and the deck crew were cleaning cement dust from the top of the cargo hatch coamings. This task had to be completed and the hatch covers replaced prior to sailing.
At about 0900, the Master was informed that the berth was required for another vessel and the vessel’s sailing time had been brought forward by about 2.5 hours. When the Master told the C/O of the revised plan, the C/O advised that he would need all available hands to complete the cleaning operation and requested that the 2/O, who was resting, be called back on deck. The 2/O arrived on deck at about 0930 and commenced sweeping cement dust from the hatch cover landing surface on the starboard side of the aft cargo hold coaming. One of the vessel’s two ABs was sweeping cement dust from the top of one of the aft hold hatch covers. The other AB and the deck cadet were working on the port side walkway, sweeping dust from the top of the forward hold coaming. The C/O was on the gantry crane, moving various hatch covers as required for the work.
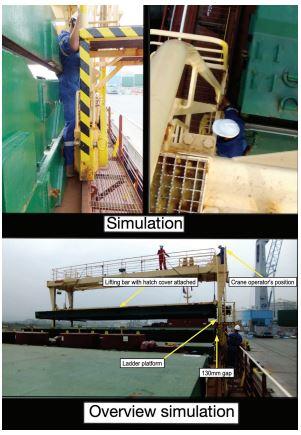
At one point, the C/O stopped the crane just short of a stack of hatch covers at the forward end of the aft hold and started to raise the crane’s lifting bar. The 2/O arrived at the forward end of the hatch cover stack. The 2/O climbed onto the cargo hatch coaming and stepped towards the gap between the crane and the stacked hatch covers. The C/O could not see the 2/O was in a dangerous position, and drove the crane aft. The 2/O screamed out in pain as he was trapped and crushed between the hatch covers and the crane’s ladder access platform. The C/O stopped and then reversed the crane. As the crane moved forward, the 2/O was rolled between the crane’s ladder platform and the hatch covers and then fell off the coaming onto the walkway below, striking his head on the guardrails on the side of the walkway.
The deck crew immediately commenced cardio-pulmonary resuscitation. About 20 minutes after the accident, two emergency medical teams, including a doctor, arrived at the scene and took over the resuscitation efforts. Later, the victim was declared deceased due to internal bleeding from organ rupture.
The investigation found, among others, that:
- The victim was crushed because he attempted to walk between the vessel’s gantry crane and a stack of cargo hold hatch covers. The C/O did not know that the victim was under the crane or what his intentions were because he was focused on raising the crane’s lifting bar.
- The toxicology report showed that the victim had more than twice the legal limit of alcohol in his bloodstream. Almost certainly the consumption of alcohol was a significant contributory factor in this accident.
- The safety culture on board the vessel was weak. Personnel were working close to moving equipment and unprotected edges, and were not wearing adequate levels of PPE. Also, alcohol consumption on a ship cannot usually go undetected. If this behaviour is tolerated then the conditions are set for a major undermining force in the safety culture on board.
Lessons learned
- Severe accidents involving gantry cranes are unfortunately not uncommon. The lessons learned from the past can be reviewed in MARS 201525, 201460 and 98058 for example.
- It goes without saying that alcohol consumption above the limits set for all mariners via STCW is to be condemned. Many companies have now adopted ‘dry-ship’ practice in order to help in the practical management of this norm.
- A strong safety culture is not a guarantee of zero accidents, but it is a bulwark against many potential bad outcomes.
- In this instance it was found that emergency stops for the gantry crane were not in sufficient number and those that were installed were badly positioned.